MENU
Home
About Us
Our Services
Submit a Claim
Resources
Work For Us
Contact Us
Accurate, Efficient,
& Deligent
Liability Claims
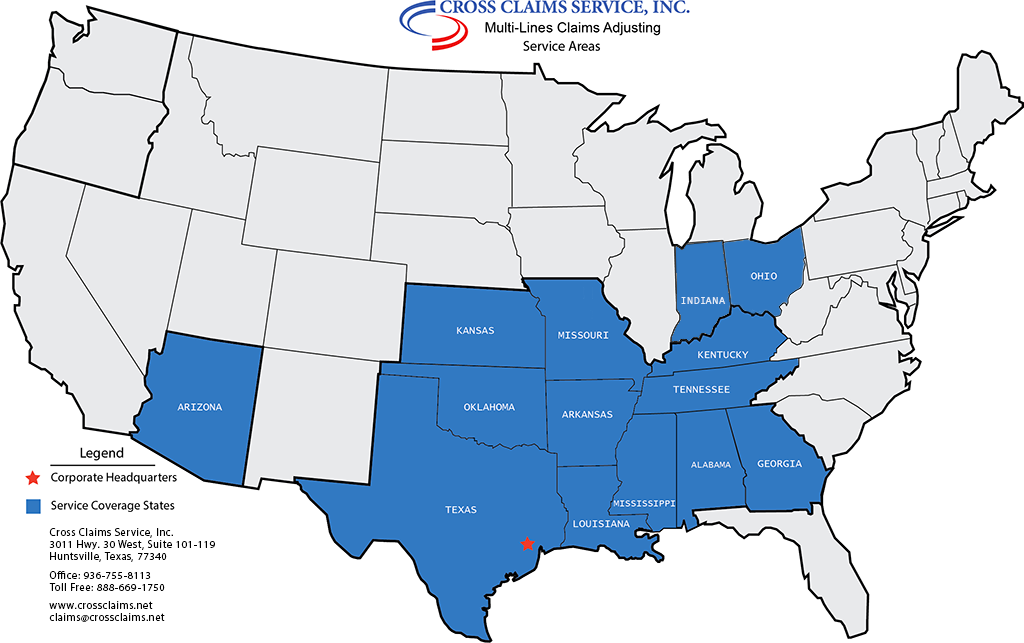
Click Here For Our Service Areas
service area
"
*
" indicates required fields
Client information
Your Name
*
Office Phone
*
Your Company
*
Address
*
Street Address
City
Alabama
Alaska
American Samoa
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Guam
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Northern Mariana Islands
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
U.S. Virgin Islands
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
Armed Forces Americas
Armed Forces Europe
Armed Forces Pacific
State
ZIP Code
Fax Number
Email
*
Claim & Assignment Details
Claim Number
*
Policy Number
Claim Type
*
Auto Liability
General Liability
Product Liability
Date of Accident or Incident
*
MM slash DD slash YYYY
Incident Involved
*
Property Damage
Bodily Injury
Financial Loss
Other
Assignment Level
*
Appraisal Only
Full Adjustment
Incident Location
*
Street Address
City
Alabama
Alaska
American Samoa
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Guam
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Northern Mariana Islands
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
U.S. Virgin Islands
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
Armed Forces Americas
Armed Forces Europe
Armed Forces Pacific
State
ZIP Code
Interviews and Statements
Do Not Contact
Insured
Claimant
Witness
Interview Only
Insured
Claimant
Witness
Written Statement
Insured
Claimant
Witness
Recorded Statemen
Insured
Claimant
Witness
Statement Summary
Insured
Claimant
Witness
Accident - Incident Description
Assignment Instructions
Policyholder / Claimant Information
Policy Holder Name
Policy Holder Contact Person
Policyholder Address
Street Address
City
Alabama
Alaska
American Samoa
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Guam
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Northern Mariana Islands
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
U.S. Virgin Islands
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
Armed Forces Americas
Armed Forces Europe
Armed Forces Pacific
State
ZIP Code
Policyholder Home Phone
Policyholder Work Phone
Policyholder Cell Phone
Claimant Name
*
Claimant Contact Person
*
Claimant Address
*
Street Address
City
Alabama
Alaska
American Samoa
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Guam
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Northern Mariana Islands
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
U.S. Virgin Islands
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
Armed Forces Americas
Armed Forces Europe
Armed Forces Pacific
State
ZIP Code
Claimant Cell Phone
*
Claimant Work Phone
Claimant Home Phone
Damage Information
Was anyone injured
No
Yes
Property Damage
No
Yes
Witnesses
No
Yes
Injured Party Details
Property Damage Details
Agent Name
Agent Phone
Comments
This field is for validation purposes and should be left unchanged.
Menu